

Community Engagement: What Is It and How Does It Help Bridge Multidisciplinary Research?
Mia DeFinoWhat is Community Engagement?
Community engagement (CE) is the collaboration between institutions of higher education and their larger communities (local, regional, state, national, and global) for the mutually beneficial exchange of knowledge and resources in a context of partnership and reciprocity. CE in the United States initially was incorporated as the mission of several land-grant universities, and starting in the 1990s, was further integrated into health promotion, or research projects to address the causes of illness in communities and developing interventions for promoting community-wide health.
CE has been referred to by many other names as the art and science have evolved over the years: participatory research, community-based participatory research, and community engaged research, among others. Yet, there are many researchers from different backgrounds including epidemiology, population health, clinical care, molecular/cell biology, and others who are just now embracing CE in practice, a trend reflected in the rise of the Clinical and Translational Science Awards, and in the growing interest of the CDC and NIH in improving the health of our nation’s communities.
CE is necessarily interdisciplinary. Translating results from the bench (discovery research) to clinical care (application) to everyday use (community) requires the collaboration and participation of individuals from many different fields of study to help address questions around health and health disparities.
A Practical Model for Community Engagement in Academic Health Centers
Some academic health centers across the country have incorporated CE as part of their mission statement, such as the Medical College of Wisconsin and the David Geffen School of Medicine at the University of California, Los Angeles, validating the scientific contribution of CE activities and programs. In the paper “Towards a practical model for community engagement: Advancing the art and science in academic health centers” by Ahmed and colleagues, a practical model for understanding CE is presented to create a foundation for researchers at academic health centers to discuss and apply the five CE components:
1) Community Outreach and Service: Community outreach is professionally related volunteer work, such as serving on the board of directors for a local organization. This is one of the most commonly reported applications of CE and provides an opportunity to make connections in the community without the community needing to make a request. By contrast, community service is personal volunteer work and often is a starting place for CE practitioners to connect with community organizations and identify meaningful issues.
2) Research: Can range from Community Engaged Research (CEnR) to Practice-based Research Networks (PBRNs) to the Patient Centered Outcomes Research Institute (PCORI). Often involves research for improving CE methods and practices as well as practices to improve the quality of clinical care in communities.
 3) Education: Spans a wide range of CE activities, such as certifications and workshops that focus on topics of interest to both academics and community partners. For example, a workshop about how to collaborate with community partners would be helpful for academics, and a workshop about how the research process works would be helpful for community partners collaborating on a research project for the first time. Service learning is another form of education that gives credit for coursework while also building relationships with community partners.
3) Education: Spans a wide range of CE activities, such as certifications and workshops that focus on topics of interest to both academics and community partners. For example, a workshop about how to collaborate with community partners would be helpful for academics, and a workshop about how the research process works would be helpful for community partners collaborating on a research project for the first time. Service learning is another form of education that gives credit for coursework while also building relationships with community partners.
4) Clinical Care: For academic health centers, this component focuses on access to free clinics, community-based care centers, and free health screening. Other institutions that do not have a medical school could focus on another asset specific to the institution.
5) Policy and Advocacy: Involves individuals from the institution advocating for public health and health policy.
Ahmed and colleagues also describe how administrative and infrastructure functions, such as promotion and tenure, risk management, evaluation, training, communication and dissemination, and financial support can help advance the art and science of the CE components at academic health centers.
For example, integrating evaluation of CE efforts at an institution is helpful for the promotion and tenure process. Historically, it has been difficult for junior faculty focused on CE research to obtain recognition for their efforts because CE is not integrated or recognized in the promotion and tenure metrics used by the committees at institutions to evaluate whether a faculty member is ready to be promoted. Another example is disseminating the results of successful CE programs to both the community and across the institution to raise awareness of the types of connections the institution has with the surrounding community. An institution’s CE activities and programs need greater recognition so that administrators and leadership can provide additional support and acknowledge the contributions of faculty and staff to improving relationships with the surrounding community. The infrastructure provides the mechanisms to evaluate these relationships and programs, and the administration can use such evaluations to make necessary changes to funding and promotion processes.
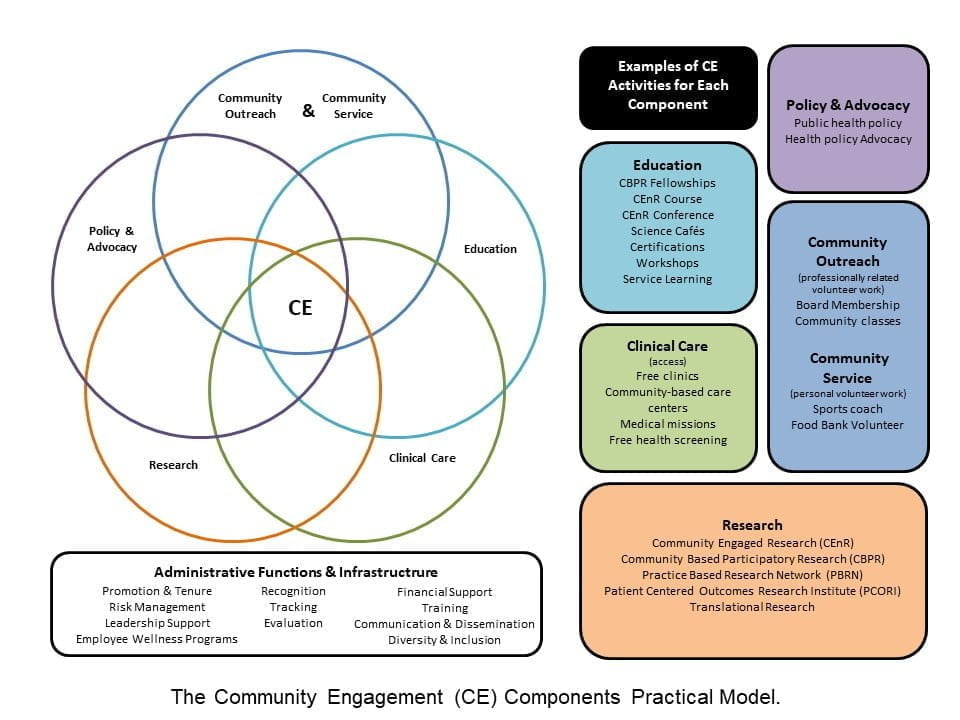
The model proposed by Ahmed and colleagues presents a list of activities for each of the five components and how those activities could overlap (see figure at right). The model is intended to help individuals and institutions understand where their strengths are for the CE components, as not all institutions will be able to support all components, and not all individuals interested in CE will be able to pursue all of them. There will be a combination of components that the institution and individuals focus on that aligns with what they do best and the needs of their community partners. The practical model for CE creates a bridge between researchers from different backgrounds who are all interested in doing research with communities, and it serves as a foundation for common understanding and discussion. Neu Young, second author on the paper, says, “The model is a way to motivate researchers and clinicians to see where their work fits in and ultimately how it advances the institution and CE mission.”
Currently, the model is of interest to institutions that want to align their CE activities with their mission and to create evaluation frameworks to measure the contributions of CE activities to their institution. Over the last several years the Medical College of Wisconsin has implemented an annual survey of their faculty and staff to assess the baseline and changes in CE activities relating to each component of the model. Currently, the team at MCW is brainstorming to develop a mechanism so that faculty and staff can report their CE activities on a regular basis, real-time tracking can be instituted, and those who are very active in CE and supporting the CE mission at MCW can be recognized. The team at MCW is open to collaboration and new approaches to implementing the model to measure the impact of institutional CE.
For more details, see Ahmed SM, Neu Young S, DeFino MC, Franco Z, Nelson DA. Towards a practical model for community engagement: Advancing the art and science in academic health centers. Journal of Clinical and Translational Science. 2017;1(5):310-315. doi:10.1017/cts.2017.304.




All comments will be reviewed and posted if substantive and of general interest to IAPHS readers.